Expanded Nursing Uganda Explanation
Abnormal Vaginal Discharge Syndrome links cause, transmission, prevention, assessment and treatment support. Good nursing notes should include infection prevention, danger signs, adherence support and community health education.
01 Abnormal Vaginal Discharge Syndrome
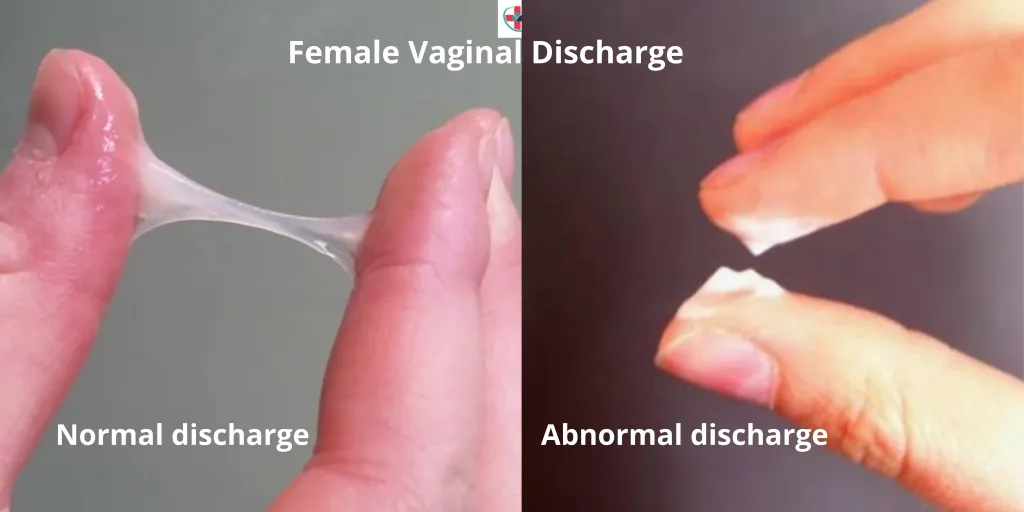
Abnormal vaginal discharge is defined as discharge that is different from usual with respect to colour/odour/consistency (e.g. discoloured or purulent or malodorous ).
While all women experience physiological vaginal discharge, concerns arise when it is perceived as abnormal. This syndrome is primarily attributed to endogenous vaginal infections, such as bacterial vaginosis and vaginal candidiasis, which are not exclusively sexually transmitted.
Candida vaginitis and bacterial vaginosis are NOT sexually transmitted diseases, even though sexual activity is a risk factor.
Case Definition:
Abnormal vaginal discharge (indicated by amount, colour, and odour) with or without lower abdominal pain or specific risk factors.
02 Aetiology:
- Vaginitis and Vaginosis : Commonly caused by bacterial vaginosis(by Gardnerella vaginalis, Mycoplasma hominis), vulvovaginal candidiasis, and trichomoniasis.
- Cervicitis : Gonococcal and chlamydial infections contribute to cervicitis, which is often asymptomatic, and rarely a cause of abnormal vaginal discharge.
03 Clinical Presentation:
All women with vaginal discharge are treated for trichomoniasis, bacterial vaginosis, and candidiasis.
Increased Quantity of Discharge, Abnormal Color, and Odor:
- Lower abdominal pain, itching, and discomfort during sexual intercourse may be reported.
- Candida Albicans Vaginitis : Characterized by a very itchy, thick, or lumpy white discharge and red, inflamed vulva.
- Trichomonas Vaginalis : Presents with an itchy, greenish-yellow, frothy discharge accompanied by an offensive smell.
- Bacterial Vaginosis : Manifests as a thin discharge with a distinct fishy odour.
Specific Discharge Characteristics for Different Infections:
- Gonorrhoea-Induced Cervicitis : Rarely causes vaginitis. Presents with purulent, thin, mucoid, slightly yellow pus discharge devoid of smell and non-itchy.
- Chlamydia-Induced Cervicitis : May present with a non-itchy, thin, colourless discharge.
Note : Microscopy and speculum examination are recommended to rule out early lesions of cervical carcinoma.
04 Management :
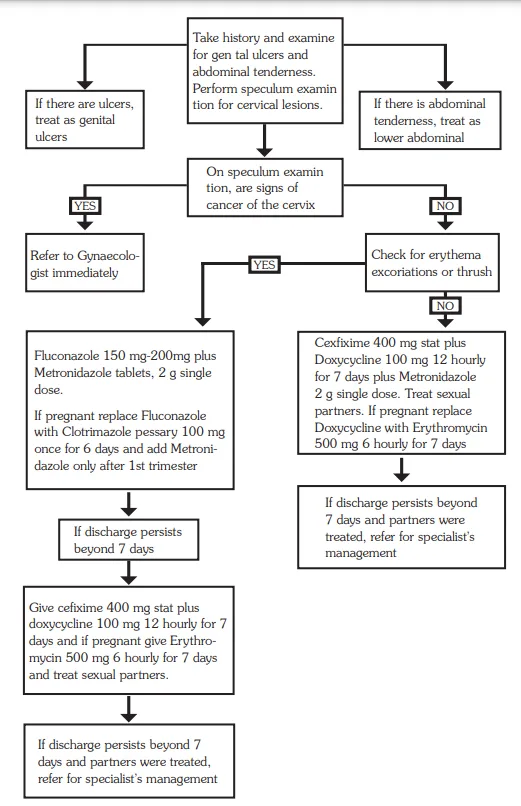
Women with vaginal discharge should be managed according to the flow chart. The flow chart differentiates between candidiasis and other vaginal discharges.
However, all women with abnormal vaginal discharge are treated for bacterial vaginosis and trichomoniasis and candidiasis. At the moment, it is not possible in this country to identify women with cervicitis, and all women with a non- curd like discharge should be treated for cervicitis.
Management Protocol for Abnormal Vaginal Discharge Syndrome:
Initial Assessment:
- Conduct a thorough history and examine for genital ulcers and abdominal tenderness.
- Perform speculum examination to check for cervical lesions.
- Assess the risk for sexually transmitted diseases.
Lower Abdominal Tenderness with Sexual Activity:
- If lower abdominal tenderness is present and the individual is sexually active, treat as per Pelvic Inflammatory Disease (PID) guidelines.
Thick, Lumpy Discharge with Itching and Erythema/Excoriations (Likely Candida):
- Administer Clotrimazole pessaries 100 mg: Insert high in the vagina once daily before bedtime for 6 days or twice daily for 3 days.
- Alternatively, prescribe Fluconazole 200 mg tablets as a single oral dose.
- Consider Metronidazole 2 g stat dose if indicated.
Abundant/Smelly Discharge (Possible Trichomonas or Vaginosis):
- Prescribe Metronidazole 2 g stat dose.
Purulent Discharge, High STD Risk, or Previous Ineffective Treatment:
Treat for Gonorrhea, Chlamydia, and Trichomonas:
- Cefixime 400 mg stat or Ceftriaxone 1g IV stat.
- Doxycycline 100 mg 12 hourly for 7 days.
- Metronidazole 2 g stat dose.
- If pregnant, replace Doxycycline with Erythromycin 500 mg every 6 hours for 7 days or Azithromycin 1 g stat.
- Ensure partner treatment.
Persistent Discharge or Dysuria Despite Partner Treatment:
- Refer the individual for further management.
Key management points include:
Treatment for Vaginal Infections:
- All women are treated for bacterial vaginosis, trichomoniasis, and candidiasis.
- Identification of cervicitis is challenging; hence, all women with non-curd-like discharge are treated for cervicitis.
Promotion of Syndromic Management Package:
- Encourage adherence to comprehensive STI management, including partner treatment, preventive measures, and health education.
Communication :
- Explain the endogenous and recurrent nature of vaginitis to patients to prevent marital discord.
- Partners with urethral discharge should be treated for cervicitis.
Evaluation and Referral:
- Persistent abnormal vaginal discharge warrants evaluation to exclude cervical cancer.
- Speculum examination and referral for specialist management may be necessary.
Counsel and educate all clients on:
- Treatment compliance.
- Condom use and provide condoms.
- Partner management.
- Offer or refer for HIV VCT services if necessary.
- Schedule a return visit.
- Abstaining from sex till symptoms resolve.
Genital Ulcer Syndrome
Click Here
05 Nursing Uganda Clinical Lens
Use Abnormal Vaginal Discharge Syndrome as a practical nursing topic, not only a memorized definition. Link cause, transmission, incubation, clinical features, treatment support and prevention.
- What to understand first: define abnormal vaginal discharge syndrome, identify the normal or expected pattern, then explain what changes when the patient is unwell.
- Why it matters in care: the nurse must recognize risk early, explain findings clearly, document accurately and know when to escalate.
- How to revise it: connect each point to assessment, nursing diagnosis or care problem, intervention, rationale and evaluation.
06 Assessment Guide
- Temperature, pulse, respiratory status, hydration, pain, rash, wounds, stool, urine or sputum changes.
- Exposure history, travel, contacts, vaccination status and comorbidities.
- Specimen orders, isolation needs, antimicrobial history and danger signs.
07 Nursing Priorities, Rationales and Outcomes
- Use standard precautions and transmission-based precautions where needed.
- Support hydration, nutrition, medicines, monitoring and early referral for severe disease.
- Teach prevention, adherence, hygiene, safe water, vector control or contact tracing as relevant.
The rationale for these priorities is patient safety: nursing actions should prevent deterioration, reduce discomfort, support recovery and create clear evidence for the next caregiver.
- Expected outcome: Symptoms improve, complications are detected early, transmission risk is reduced and treatment is completed correctly.
08 Patient Teaching and Revision Check
- Explain abnormal vaginal discharge syndrome in simple language the patient or caregiver can repeat back.
- Teach warning signs, medicine or follow-up instructions, hygiene or lifestyle points where relevant.
- For exams, prepare a short answer using: definition, causes or risk factors, signs, assessment, management, complications and prevention.
- For ward practice, document baseline findings, actions taken, patient response and the plan for review.
Illustrations and Diagrams (4)


Related Video Lectures
Watch nursing lecture videos on YouTube for this topic. Opens in a new tab.
Watch on YouTubeExternal link: YouTube may use its own cookies and terms. Nursing Uganda is not affiliated with YouTube.