Expanded Nursing Uganda Explanation
Hypercalcemia should be understood beyond a short definition. Link the concept to patient history, focused assessment, common risks, nursing priorities, documentation and evaluation of outcomes.
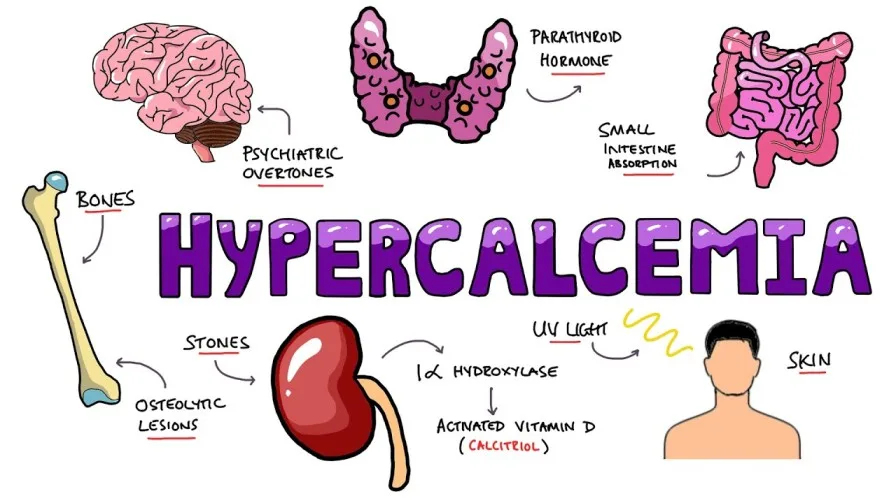
01 Hypercalcemia
Hypercalcemia is a threatening metabolic disorder associated with cancer. It commonly occurs in patients with breast cancer, multiple myeloma, and head, neck, and renal tumors.
Hypercalcemia associated with malignancy is referred to as Hypercalcemia of Malignancy (HCM) and is commonly associated with primary cancers of the
- breast
- lungs
- neck
- kidney
- esophagus
- gastrointestinal tract
- cervix, leukemia
- multiple myeloma, and melanomas.
HCM most often results from bone metastasis. There is a release of calcium from the bones, which causes hypercalcemia. Additionally, cancer treatment modalities such as estrogen and anti-estrogen agents are associated with the development of HCM.
Non-cancer related factors associated with the development of hypercalcemia include
- immobility
- dehydration
- excessive intake of calcium and Vitamin D
- decreased parathyroid hormone levels, and vitamin A intoxication.
02 Causes :
- Specific cancers: Certain types of cancer, such as breast cancer, lung cancer, kidney cancer, leukemia, multiple myeloma, and melanomas, are commonly associated with hypercalcemia. The presence of these cancers can lead to the release of calcium from the bones, contributing to elevated calcium levels in the bloodstream.
- Treatment modalities: Cancer treatment methods, including the use of estrogen and anti-estrogen agents, can be associated with the development of hypercalcemia. These treatment modalities may impact calcium regulation in the body and contribute to increased levels of calcium in the blood.
- Non-malignant causes: Hypercalcemia can also occur due to non-cancer-related factors. These may include immobility, dehydration, excessive intake of calcium and Vitamin D, decreased levels of parathyroid hormone, and vitamin A intoxication. These factors can disrupt the normal balance of calcium in the body and lead to elevated levels.
- Lytic bone lesions: In some cases, hypercalcemia can be caused by lytic bone lesions. These are bone abnormalities characterized by the destruction of bone tissue. When bone lesions are present, calcium is released from the bones into the bloodstream, contributing to hypercalcemia. Additionally, there may be a decrease in the excretion of urinary calcium, further elevating calcium levels.
03 Signs and symptoms:
- General malaise : Patients with hypercalcemia may experience a general sense of discomfort, uneasiness, or fatigue.
- Nausea and vomiting : Hypercalcemia can cause nausea and vomiting, leading to gastrointestinal disturbances.
- Anorexia : Loss of appetite or decreased desire to eat can occur in individuals with hypercalcemia.
- Constipation : Elevated calcium levels can affect the smooth muscle contractions in the gastrointestinal tract, leading to constipation and difficulty passing stool.
- Bone pain : Hypercalcemia can cause bone pain, which may be localized or generalized throughout the body. This pain is often a result of the underlying bone abnormalities or metastasis.
- Thirst and polyuria : Increased thirst and excessive urination (polyuria) can be signs of hypercalcemia, as the body tries to eliminate excess calcium through increased fluid intake and urine output.
- Polydipsia : Polydipsia refers to excessive thirst, which can be experienced by individuals with hypercalcemia.
- Severe dehydration : Hypercalcemia can lead to dehydration due to increased fluid loss through urine and other symptoms like vomiting and decreased oral intake.
- Drowsiness : Excess calcium in the bloodstream can affect the central nervous system, leading to drowsiness and excessive sleepiness.
- Confusion and coma : Severe hypercalcemia can cause neurological symptoms, including confusion and, in extreme cases, coma.
- Cardiac arrhythmias : Elevated calcium levels can disrupt the normal electrical activity of the heart, leading to irregular heart rhythms or arrhythmias.
- Mental state changes : Hypercalcemia can affect mental functioning, leading to changes in concentration, memory, mood, and irritability.
- Hallucinations : In some cases, hypercalcemia can cause hallucinations, which are perceptual distortions or false sensory experiences.
- Jumbled speech : Speech abnormalities, such as slurred speech or difficulty finding the right words, can occur in individuals with hypercalcemia.
- Depression and fatigue : Hypercalcemia can contribute to feelings of depression and persistent fatigue.
- Patients may report visual changes: Some individuals with hypercalcemia may experience visual changes, such as blurring, double vision, or sensitivity to light.
04 Diagnosis and Investigations:
- Medical History and Physical Examination: A thorough medical history and physical examination are important in identifying potential risk factors and assessing the symptoms associated with hypercalcemia.
- Serum Calcium Level : Measurement of serum calcium levels is a primary diagnostic tool for hypercalcemia. A serum calcium level greater than 2.60 mmol/dL is indicative of hypercalcemia.
- Ionized Calcium : In some cases, measuring ionized calcium levels may provide a more accurate assessment of calcium abnormalities.
- Parathyroid Hormone (PTH) Level : Measuring PTH levels can help differentiate between different causes of hypercalcemia. In primary hyperparathyroidism, PTH levels are typically elevated, while in malignancy-associated hypercalcemia, PTH levels are usually suppressed.
- Kidney Function Tests: Assessing kidney function is important as hypercalcemia can affect renal function. Tests such as blood urea nitrogen (BUN) and creatinine levels help evaluate renal function.
- Serum Phosphate and Magnesium Levels: Measuring phosphate and magnesium levels can provide additional information about the underlying causes of hypercalcemia.
- 24-Hour Urine Calcium : Collecting a 24-hour urine sample for calcium measurement helps evaluate urinary calcium excretion and can assist in determining the cause of hypercalcemia.
- Imaging Studies: Imaging techniques such as X-rays, bone scans, computed tomography (CT), or magnetic resonance imaging (MRI) may be conducted to identify any bone abnormalities or metastases.
- Additional Investigations : Depending on the clinical presentation and suspected underlying cause, additional investigations such as complete blood count (CBC), liver function tests, measurement of serum protein electrophoresis, and assessment of vitamin D levels may be performed.
05 **Management**
- Hydration : Intravenous rehydration and close monitoring are key aspects of treating hypercalcemia. Hydration helps to reverse the decrease in intravascular volume. In cases of mild hypercalcemia, rehydration with normal saline at a rate of 100-120 ml/hr is often sufficient.
- Medications : Bisphosphonates are commonly used to inhibit osteoclastic bone reabsorption and lower calcium levels. In cases of moderate to severe hypercalcemia, the treatment approach includes rehydration as mentioned above, followed by the administration of bisphosphonates. One example of a bisphosphonate is Pamidronate. It’s important to ensure adequate hydration before giving bisphosphonates, and the dose may need to be repeated every 3-4 weeks. However, it’s worth noting that bisphosphonates may not be readily available in resource-poor countries due to their cost.
Mild hypercalcemia
- Step 1: R ehydrate with normal saline 100-120ml/hr.; this alone is sufficient in small number of cases.
Moderate to severe hypercalcemia
- Step 1 : as above
- Step 2 : bisphosphonates; e.g. Pamidronate, (not usually available in resource poor countries because they are expensive) Reduce calcium if given IV. Care must be taken to rehydrate the well prior to administration of bisphosphonates. The dose may need repeating 3-4 weekly.
- Corticosteroids may lower the calcium in hematological malignancies but less effective in solid tumor.
- End-of-life care : In cases where bisphosphonates are not available or hypercalcemia indicates the terminal phase of the disease, the focus shifts to providing comfort and dignity to the patient.
- Simple measures like
- regular mouth care,
- bowel care,
- regular turning of the patient,
- effective pain and symptom control are important in ensuring a dignified and comfortable end-of-life experience.
06 For HCM;
Management and Care:
- The management of Hypercalcemia of Malignancy (HCM) may involve treating the underlying malignancy. This could include chemotherapy , radiation therapy, and/or surgery, depending on the specific cancer.
- Hydration: Patients should aim to consume 1 to 2 liters of fluids per day, if they can tolerate oral fluids.
- Fluid Replacement: For patients with moderate to severe HCM (calcium levels above 13 mg/dL), fluid replacement may be necessary to restore extracellular fluid balance. This typically involves administering 5 to 10 liters of fluid.
- Saline Administration: In cases of dehydration or severe hypercalcemia, the administration of saline may be required to restore volume and correct electrolyte imbalances.
- Corticosteroid Therapy: Patients with HCM caused by steroid-responsive tumors may benefit from corticosteroid treatment. Corticosteroids can help lower calcium levels in these cases.
- Symptom Management and Mobility: Management of HCM also involves addressing symptoms associated with hypercalcemia and promoting mobility. This may include medications to alleviate bone pain, such as nonsteroidal anti-inflammatory drugs ( NSAIDs ), and implementing strategies to improve patient comfort and mobility.
- Constipation Assessment and Treatment: Patients should be assessed for constipation, as it can be a common symptom of hypercalcemia. If constipation is present, appropriate measures should be taken to alleviate it.
07 Nursing Uganda Clinical Lens
Use Hypercalcemia as a practical nursing topic, not only a memorized definition. Focus on comfort, dignity, symptom control, communication and family support.
- What to understand first: define hypercalcemia, identify the normal or expected pattern, then explain what changes when the patient is unwell.
- Why it matters in care: the nurse must recognize risk early, explain findings clearly, document accurately and know when to escalate.
- How to revise it: connect each point to assessment, nursing diagnosis or care problem, intervention, rationale and evaluation.
08 Assessment Guide
- Pain and other symptoms, function, sleep, appetite, mood, spiritual distress and family concerns.
- Medication response, side effects, wound or skin needs and end-of-life preferences.
- Caregiver burden, home resources and urgent red flags.
09 Nursing Priorities, Rationales and Outcomes
- Relieve distressing symptoms and prevent avoidable suffering.
- Communicate honestly, respectfully and at the patient's pace.
- Support family care, medication access, dignity and continuity.
The rationale for these priorities is patient safety: nursing actions should prevent deterioration, reduce discomfort, support recovery and create clear evidence for the next caregiver.
- Expected outcome: Symptoms are better controlled, patient preferences are respected and the family knows when to seek help.
10 Patient Teaching and Revision Check
- Explain hypercalcemia in simple language the patient or caregiver can repeat back.
- Teach warning signs, medicine or follow-up instructions, hygiene or lifestyle points where relevant.
- For exams, prepare a short answer using: definition, causes or risk factors, signs, assessment, management, complications and prevention.
- For ward practice, document baseline findings, actions taken, patient response and the plan for review.
Illustrations and Diagrams (3)


Related Video Lectures
Watch nursing lecture videos on YouTube for this topic. Opens in a new tab.
Watch on YouTubeExternal link: YouTube may use its own cookies and terms. Nursing Uganda is not affiliated with YouTube.