Expanded Nursing Uganda Explanation
Genital Ulcer Syndrome should be reviewed through safe maternal and newborn assessment, early recognition of danger signs, respectful communication and timely referral. Connect the definition to vital signs, bleeding, fetal or newborn wellbeing, patient education and local protocol requirements.
01 Genital Ulcer Syndrome
Genital ulcer disease is a common syndrome affecting both men and women, characterized by single or multiple ulcers with different clinical manifestations.
Case Definition:
Non-vesicular Genital Ulcer : Ulcer on the penis, scrotum, or rectum in men, and on the labia, vagina, or rectum in women, with or without inguinal adenopathy. Vesicular ulcers involve the presence or history of vesicles.
02 Causes :
The aetiology of this syndrome varies across geographical regions and can evolve over time, often presenting challenges due to mixed infections and the influence of HIV.
- Non-vesicular Ulcers: Commonly caused by syphilis, chancroid, lymphogranuloma venereum, granuloma inguinale, or atypical cases of genital herpes (HSV infection).
- Vesicular Ulcers : Primarily caused by Herpes genitalis, syphilis, and Chancroid in Uganda.
Multiple organisms can cause genital sores, commonly:
- Treponema pallidum bacteria: syphilis
- Herpes simplex virus: genital herpes
- Haemophilus ducreyi: Chancroid
- Donovania granulomatis: Granuloma inguinale
- Chlamydia strains: lymphogranuloma venereum (LGV)
03 Clinical Presentation:
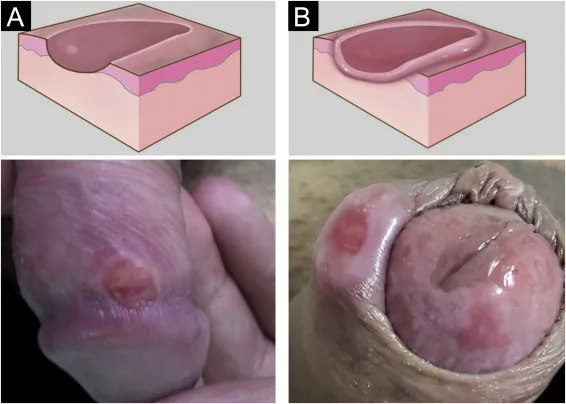
In men, genital ulcer disease occurring under the prepuce may present with a discharge in uncircumcised male patients, therefore, prepuce should be retracted and examined for ulcer lesions.
Female patients should have the labia separated and inspected, with speculum examination if necessary.
Mixed infections are common
- Primary syphilis : the ulcer is at first painless and may be between or on the labia or on the penis.
- Secondary syphilis : multiple, painless ulcers on the penis or vulva.
- Genital Herpes : small, multiple, usually painful blisters, vesicles, or ulcers. Often recurrent.
- Granuloma inguinale : an irregular ulcer which increases in size and may cover a large area.
- Chancroid : multiple, large, irregular ulcers with enlarged painful suppurating lymph nodes.
04 Management :
Prompt treatment is important due to the increased risk of HIV transmission associated with genital ulcers.
Treatment strategies for both genders should align with the local epidemiology. In Uganda, the following approach is recommended:
- Non-vesicular Ulcers : Treatment according to the provided flow chart , distinguishing between specific etiologies.
- Vesicular Ulcers: Given the increased risk of HIV transmission, treatment for genital herpes is strongly recommended.
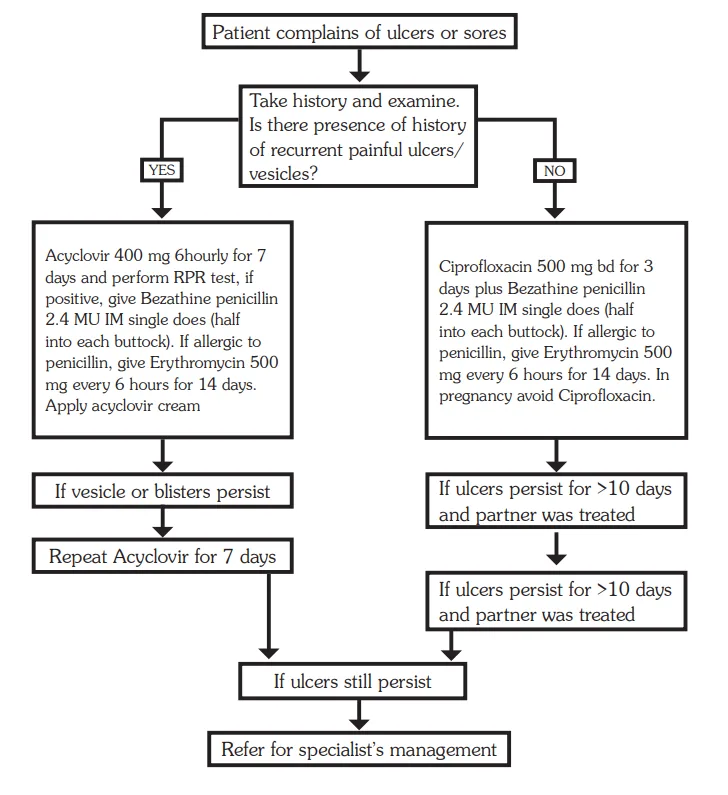
Management Protocol for Genital Ulcer Syndrome:
Multiple Painful Blisters or Vesicles (Likely Herpes):
- Administer Aciclovir 400 mg every 6 hours for 7 days.
- If RPR (Rapid Plasma Reagin) positive, add Benzathine penicillin 2.4 MU IM single dose (half in each buttock).
- In case of persistent lesions, repeat Acyclovir for an additional 7 days.
All Other Cases:
- Prescribe Ciprofloxacin 500 mg every 12 hours for 3 days.
- Add Benzathine penicillin 2.4 MU IM single dose (half in each buttock).
- For individuals with penicillin allergy, substitute with Erythromycin 500 mg every 6 hours for 14 days.
If Ulcer Persists Beyond 10 Days and Partner Was Treated:
- Add Erythromycin 500 mg every 6 hours for 7 days.
If Ulcer Still Persists:
- Refer the individual for specialist management.
Important Notes:
- A negative RPR does not exclude early syphilis.
- Genital ulcers may appear with enlarged and
- fluctuating inguinal lymph nodes (buboes). Do not incise buboes.
Other Components of STI Case Management:
In addition to antimicrobial therapy, comprehensive STI case management includes:
- Partner Notification and Treatment: Partners should be notified and treated, irrespective of symptoms.
- Preventive Measures: Emphasize preventive measures, including safe sexual practices and condom use.
- Health Education : Counsel and educate all clients on:
- The importance of treatment compliance and regular follow-ups.
- Condom use and provide condoms.
- Partner management.
- Offer or refer for HIV VCT services if necessary.
- Schedule a return visit if feasible.
- Abstaining from sex symptoms resolve.
05 Inguinal Buboes Syndrome
Click Here
06 Nursing Uganda Clinical Lens
Use Genital Ulcer Syndrome as a practical nursing topic, not only a memorized definition. Link cause, transmission, incubation, clinical features, treatment support and prevention.
- What to understand first: define genital ulcer syndrome, identify the normal or expected pattern, then explain what changes when the patient is unwell.
- Why it matters in care: the nurse must recognize risk early, explain findings clearly, document accurately and know when to escalate.
- How to revise it: connect each point to assessment, nursing diagnosis or care problem, intervention, rationale and evaluation.
07 Assessment Guide
- Temperature, pulse, respiratory status, hydration, pain, rash, wounds, stool, urine or sputum changes.
- Exposure history, travel, contacts, vaccination status and comorbidities.
- Specimen orders, isolation needs, antimicrobial history and danger signs.
08 Nursing Priorities, Rationales and Outcomes
- Use standard precautions and transmission-based precautions where needed.
- Support hydration, nutrition, medicines, monitoring and early referral for severe disease.
- Teach prevention, adherence, hygiene, safe water, vector control or contact tracing as relevant.
The rationale for these priorities is patient safety: nursing actions should prevent deterioration, reduce discomfort, support recovery and create clear evidence for the next caregiver.
- Expected outcome: Symptoms improve, complications are detected early, transmission risk is reduced and treatment is completed correctly.
09 Patient Teaching and Revision Check
- Explain genital ulcer syndrome in simple language the patient or caregiver can repeat back.
- Teach warning signs, medicine or follow-up instructions, hygiene or lifestyle points where relevant.
- For exams, prepare a short answer using: definition, causes or risk factors, signs, assessment, management, complications and prevention.
- For ward practice, document baseline findings, actions taken, patient response and the plan for review.
Illustrations and Diagrams (2)
Related Video Lectures
Watch nursing lecture videos on YouTube for this topic. Opens in a new tab.
Watch on YouTubeExternal link: YouTube may use its own cookies and terms. Nursing Uganda is not affiliated with YouTube.